



New partnership with Cisco and Grampians Health to upskill healthcare sector
RMIT’s Health Transformation Lab and College of Vocational Education are piloting a program to rapidly upskill front-line staff, broader health workforce and IT professionals in the healthcare sector to meet the industry’s emerging skills needs.

Right to housing event shines a light on Australia’s housing crisis
In a thought-provoking event hosted by RMIT University, a panel of experts addressed the growing issue of housing rights in Australia.

New report proposes using tax system to improve rental properties
A new report from RMIT University urban policy experts recommends using Australia’s tax system to force investors to improve conditions for private renters.
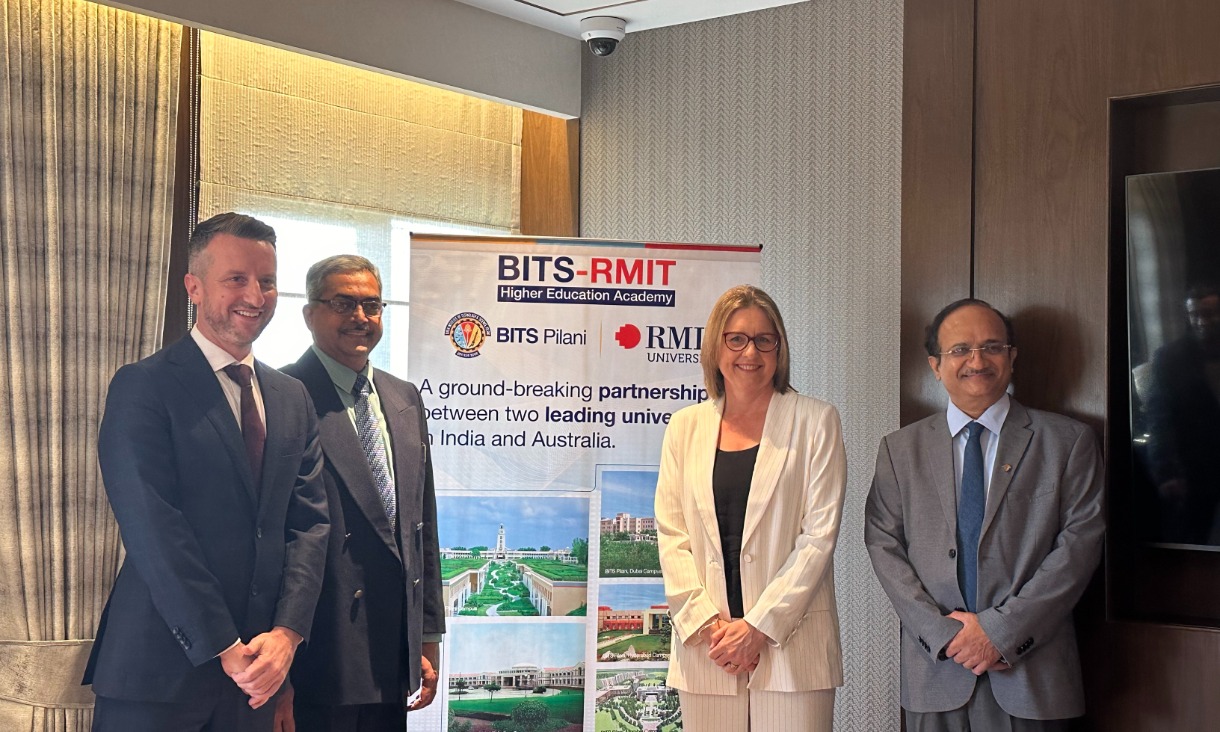
Victorian Premier joins RMIT to celebrate innovative India-Australia higher education partnership
The Victorian Premier has joined executives from the Birla Institute of Technology and Science and RMIT University to meet students of the BITS-RMIT Higher Education Academy and learn more about their experiences.